Whether it is visiting a doctor, understanding and paying a medical bill, or picking out the right health insurance plan, we can probably all agree that our regular interactions with the healthcare system are not as seamless or as easy to access as they should be. Healthcare is too hard to navigate, costs too much, and ultimately does not work well for the people it’s meant to serve — all of us.
Too often, this lapses into pessimism, a belief that we can’t improve US healthcare. At nearly one-fifth of the economy, healthcare is too big to fail — and to fix. But the truth is that there is a lot that people can change in healthcare if they are motivated to take on these seemingly insurmountable problems.
The trick is to think like a basketball team, not a track team. In the latter, runners are out for themselves, and points are awarded for individual performance. In basketball, nearly every point scored relies on the skills and effort of the whole team. Assists are as important as goals scored, and strong defense makes offensive success possible.
Creating this collaborative environment takes embracing three principles: servant leadership, connectedness through authenticity, and innovating with transparency.
Servant Leadership
First, at the heart of everything is servant leadership. Servant leadership is all about keeping the people that you serve at the core of what you do. At Walgreens, our boots-on-the-ground leaders are our pharmacists. Walgreens pharmacists are in nearly 9,000 stores across the country, and especially in rural communities, pharmacists are the cornerstone of people’s perceptions of the healthcare system.
Our pharmacists embody servant leadership. Often, they are providing expert counsel while integrating kindness and compassion into every interaction they have with their community. Their servant leadership perspective prompts our pharmacists to truly go above and beyond for patients. Our pharmacists serve as the healthcare system’s air traffic control by coordinating care, knitting together patient needs, and following up to make sure those needs are taken care of. Walgreens pharmacists also help with minor injuries or illnesses and deliver care through vaccination, testing, and, in some cases, prescribing.
Our pharmacists are truly connected to their communities, and they find ways where they can really help and make a difference. Their servant leadership mentality motivates them to do so, and that culture feeds up into the entire Walgreens organization.
Connectedness Through Authenticity
While servant leadership can create connections to the community, it’s also important to make internal connections that strengthen teams. Authentic leadership is hard to crystalize and almost impossible to rehearse, but when it’s not there, teams fall apart. Team members have to know that their leader has passion and has their back. More importantly, team members have to believe that their leader has heart and kindness in an authentic way. If the passion isn’t genuine, it’s obvious. But when authentic leadership is there, it’s a key differentiator.
When I was in military training, I was interacting with people who had graduated from military schools and places like West Point — they were much better equipped to take on the technical and logistical tasks of our training. I wasn’t the best at many of the military skills themselves, like loading weapons or excelling on drills, but in a leadership position, I was awarded for showing heart and passion, conveying that to my organization, and taking care of my team. That created connectivity and trust among all of us.
To me, that kind of magic happens when leaders and teams find a collective purpose and trust each other to achieve that purpose. This trust facilitates what General Stanley McChrystal calls in his book, Team of Teams, “shared consciousness,” or thinking and acting as a team rather than as individuals.
In healthcare, for example, we have a collective purpose, but we don’t always have trust between stakeholders or from our patients. To be better leaders in our teams and across the industry, we have to get back to basics — show authenticity, connect to our common purpose, and trust our teammates as we all work towards our goal of serving patients and improving quality of life.
Innovating with Transparency
The best leaders cultivate servant leadership and create authentic connections to tie their team together, but they also keep innovating. Many leaders and organizations focus on innovation, but what takes innovation from a buzzword to the next level is changing paradigms with clear goals and transparent communication.
No team or organization stays stagnant forever — nor should we want it to. Particularly in healthcare, change happens quickly, and organizations that don’t adapt technology effectively are often left behind. At the same time, change can feel scary and uncertain for teams, especially today when conversations about new technologies like artificial intelligence are also accompanied by discussions of how many jobs AI will replace.
During times of change, transparency in leadership takes precedence. That’s why, at Walgreens, we’re being thoughtful about where our existing strengths are — our servant leaders, our people — and how AI can complement what they do. Instead of spending time counting pills and doing paperwork, AI can help our pharmacists facilitate human connection by freeing time to really listen to people, understanding their health concerns so we can treat them better. Without transparent leadership about new technology, teams fall into fear. Strategic application of technology and open communication can help teams thrive.
Thank you for reading the Innovative Leadership Insights, where we bring you thought leaders and innovative ideas on leadership topics each week. We strive to elevate the quality of leadership worldwide. If you are looking for help developing your leaders, explore our services.
https://www.innovativeleadershipinstitute.com/wp-content/uploads/2022/03/ILI-Anniversary-Logo.png00Devon Mushalkohttps://www.innovativeleadershipinstitute.com/wp-content/uploads/2022/03/ILI-Anniversary-Logo.pngDevon Mushalko2024-02-08 10:08:072024-03-04 10:57:43Dispensing Wellness: Walgreens’ Rx for Healthcare
The article was published in an Appendix to the recently released Innovative Leadership in Health Care book by Maureen Metcalf of Innovative Leadership Institute and Erin S. Barry, M.S; Dukagjin M. Blajak, M.D., Ph.D.; Suzanna Fitzpatrick, DNP; Michael Morrow-Fox, M.B.A., Ed. S.; and Neil E. Grunberg, Ph. D. It provides healthcare workers with frameworks and tools based on the most current research in leadership, psychology, neuroscience, and physiology to help them update or innovate how they lead and build the practices necessary to continue to update their leadership skills. It is provided as a companion to the podcast with Eric Douglas Keene on Diversity Recruiting: Changes and Retention.
I have strong memories of an eye-opening conversation I had with some friends when I began work in a suburban hospital. I met my friend and his wife for a snack at the hospital cafeteria when they visited for his routine physical. I teased him about how nice he was dressed. He looked at his wife and then back at me. He smiled as he replied, “We have to dress up when we go to this hospital,” he said. “Otherwise, the security staff wants to escort us to our physician’s office.” After that conversation, I noticed several instances of African American patients, families, and staff receiving ‘special help’ from the hospital security staff. I was taken aback at both the hospital’s racist institutional behavior and my complete obliviousness to the racism.
This section is about innovative leadership for JEDI. Innovative leadership for JEDI refers not to STAR WARS mind control techniques, but the other JEDI—[Social] Justice, Equity, Diversity, and Inclusion. Innovative leadership for JEDI is the ability to impact individuals, teams, and systems to create a fair and engaging health care organization. For patients. For families. For health care workers. Of all backgrounds, genders, colors, and beliefs. The Innovative Leadership JEDI section is divided into three subsections. Bias and health care, the health care crisis resulting from bias, and a pathway for leaders to address the JEDI health care crisis in their organizations.
Bias and Health Care
Our experiences are that most health care organizations and most health care leaders try to create a welcoming JEDI environment. Most health care organizations and leaders truly value the principles of JEDI. Research and experience, however, reveals too many health care organizations that are unwelcoming and un-inclusive. In the absence of malice, how does a health care organization create an unwelcoming and un-inclusive environment? We submit the answer may lie in cognitive biases that allow organizations and leaders to believe a problem exists, but… “It’s not me and not us.”
Emily Pronin notes, “Human judgment and decision making is distorted by an array of cognitive, perceptual and motivational biases.” Most health care professionals receive training in statistical practices aimed at eliminating biases in clinical practice. Pronin goes on to describe a phenomenon termed blindspot bias writing, “Recent evidence suggests that people tend to recognize (and even overestimate) the operation of bias in human judgment – except when that bias is their own.”
Banaji and Greenwald have further described the blindspot bias as a bias people can readily see in others but have great difficulty seeing in themselves. Blindspot biases manifest in statements like, “I know there is a lot of racial prejudice in the world, but I don’t see color, only people,” or, “I know most people that don’t understand cultural norms can be offensive, but I understand respect, so I am never offensive in any culture.” When someone is aware that a phenomenon regularly exists in others but denies the possibility that it could exist in them, a blindspot bias may be the reason for their confidence. In the health care world, it is often misguided confidence that may dehumanize and disenfranchise others.
In addition to the blindspot bias, health care leaders can suffer from implicit biases. Harvard University’s Project Implicit describes implicit biases as, “attitudes and beliefs that people may be unwilling or unable to report.” Project Implicit provides the example of an implicit bias as, “You may believe that women and men should be equally associated with science, but your automatic associations could show that you (like many others) associate men with science more than you associate women with science.”
Mission statements and Diversity Departments in health care organizations echo a call to deliver the highest possible care and adherence to the value principles of JEDI. This in contrast to the many patients, families, employees, and communities suffering consequences of social injustice, inequity, lack of diversity, and un-inclusiveness. The combination of blindspot and implicit biases create a JEDI crisis in our health care systems. A crisis that hides in plain view through a cloak of “not me, not us” beliefs.
The Tale of a JEDI Health Care Crisis
The evidence on JEDI and health care delivery highlights systemic failures on almost every level. Below are a few health care statistics illustrating the breakdown of principles of JEDI for our patients, their families, and our employees:
During the first ten months of the Covid-19 crisis, U.S. data from the COVID Racial Data Tracker showed mortality rates 150% higher for African Americans, 135% higher for Indigenous American People, and 125% for Hispanic Americans than for White Americans. Bassett and colleagues reported that African Americans between the ages of 35 and 44 had nine times higher mortality rates than their White American counterparts.
Marcella Nunez-Smith and colleagues found nearly one in three Black physicians, nearly one in four Asian physicians, and one in five Hispanic/Latino physicians have left at least one job due to discriminatory practices.
Dickman and colleagues note the top one percent of affluent males live on average 15 years longer than the lowest one percent of poor males. Low-income families are in poor health at rates 15 percent higher than their affluent American counterparts.
Using U.S. Census Data, The Center for American Progress reports women in the workforce earn $.77 for every dollar their male counterparts earn. Women are often pigeonholed into “pink-collar” jobs, which typically pay less. Forty-three percent of the women employed in the United States are clustered in just 20 occupational categories, of which the average annual median earnings is less than $29,000.
The Organisation for Economic Co-operation and Development reports that female physicians make up only 34 percent of all U. S. physicians.
More than 25 percent of African American women and nearly 25 percent of Hispanic American women live in poverty. Elderly women have poverty rates over double those of elderly men.
The Center for American Progress reports more than 10 percent of African Americans and more than 16 percent of Hispanic Americans are uninsured compared to 5.9 percent of White Americans.
African American adults over age 20 suffer from hypertension at the rate of 42 percent compared to 29 percent for White American adults.
In a survey of over 27,000 transgender respondents, Herman and colleagues reported, “In the year prior to completing the survey, one-third (33%) of those who saw a health care provider had at least one negative experience related to being transgender, such as being verbally harassed or refused treatment because of their gender identity.”
A survey of over 40,000 LGBTQ Americans aged 13 to 24 by The Trevor Project found almost half of the respondents engaged in self-harm. And 40 percent have “seriously considered” attempting suicide—in just the past year.
Ronald Wyatt reports, “The total cost of racial/ethnic disparities in 2009 was approximately $82 billion—$60 billion in excess healthcare costs and $22 billion in lost productivity. The economic burden of these health disparities in the US is projected to increase to $126 billion in 2020 and to $353 billion in 2050 if the disparities remain unchanged.”
JEDI Innovative Health Care Leadership Action
Reading the statistics above and the myriad of statics available, we find it hard to deny a systemic failure of the health care delivery system and our health care organizations. How did it get this bad when we have so many well-intended and highly skilled leaders? Blindspot and implicit biases can cause inaction in an otherwise effective leadership team. Leaders with blindspot and implicit biases do not disregard problems; they render problems moot through the belief, “not me, not us.” We hope the shortlist of statistics above brings some awareness that “me/we” are both the health care problem and the solution.
Innovative health care leaders can change the course of social injustice, inequity, lack of diversity, and un-inclusion. Using their influence, leaders can take an evidence-based approach to JEDI, learn/teach cultural competence, practice cultural humility, create support for diverse populations, and grow communities to change the course of this systemic failure. We elaborate with some definitions and examples below.
Pfeffer and Sutton wrote, “A bold new way of thinking has taken the medical establishment by storm in the past decade: the idea that decisions in medical care should be based on the latest and best knowledge of what actually works.” Pfeffer and Sutton went on to write while the idea of evidence-based care is almost uncontested, physicians only make evidence-based decisions 15 percent of the time. This is certainly of concern for clinical decision-making, and it is an equal concern for changing the tide of systemic JEDI failures.
As leaders, we must ask, “How would someone with a blindspot or implicit bias know if women, minorities, or people of non-traditional identities are experiencing injustice, inequity, or un-inclusion?” The answer is evidence. Do job applicants with the names Julio and Jamal have the same employment opportunities as applicants with the names John and James? Do our women and minority workers make comparable wages to our white male workers? Do immigrant patients feel respected when receiving care? Are our employees reflective of the community in which we reside? We are uncertain without evidence. Without evidence, our instincts and experiences guide us; instincts and experiences which can be skewed by biases.
Innovative JEDI leaders (like you) are actively pursuing evidence that their organizations are socially just, equitable, appropriately diverse, and inclusive. Evidence—accurate data that is analyzed and understood; confirms or denies the existence of JEDI. If a leader does not have JEDI evidence, the “not me and not us” biases may predominate the institutional consciousness.
Cultural learning opportunities should be readily available in your organization. Cultural competence, the ability to recognize, appreciate, and interact successfully with people from other cultures, is essential for any healthcare professional. In addition, Tervalon and Murray-Garcia observed, “Cultural humility incorporates a lifelong commitment to self-evaluation and self-critique, to redressing the power imbalances in the patient-physician dynamic, and to developing mutually beneficial and nonpaternalistic clinical and advocacy partnerships with communities on behalf of individuals and defined populations.” Innovative leaders teach, support, and model cultural humility within their organizations.
We have had many conversations with health care human resource professionals observing, “We get minority candidates hired, we just can’t get them to stay.” When diverse employees walk into a room with people who do not look like them, do not believe like them, may have preconceived negative ideas about people like them, it can be overwhelming. Patients, their families, and employees need to feel the organization’s support, receive mentoring on the navigation of differences, and understand that their differences are vital for the community and organization’s strength. Innovative leaders forge pathways of support for inclusion, mentorship, and engagement in their health care organizations. Support groups, mentoring programs, organizational messages, and evidence gathering serve to support and retain diverse populations.
Innovative leaders look at the gaps in their communities and think about how to close those gaps. In an article entitled, Physicians for Social Justice, Diversity and Equity: Take Action and Lead, Lubowitz and colleagues note, “Few orthopedic surgeons are minorities or female, and orthopedic surgery is not perceived to be an inclusive specialty. This is an obstacle to equitable diverse hiring.” Despite the lack of diverse candidates in the profession, Lubowitz and colleagues passionately express the need to advocate, inspire, and continuously improve as a profession.
We agree. If there are gaps in finding physicians and other health care employees that are reflective of the community, start programs to recruit, train, and inspire the community. Programs from elementary school to advanced educational grants can all serve to change a community. Lubowitz and colleagues recommend, “In terms of minorities and women making a choice to pursue medicine and then orthopedic surgery as a desired medical specialty, we wield enormous impact and a most direct influence. We must consciously change our behavior and demonstrate that we are an inclusive medical specialty.” Every innovative health care leader can demonstrate support for inclusion.
Most of us have experienced the patient that demands, “I’m sorry, but I don’t want a [Female, Jewish, Muslim, Gay, Old, Younge, Black, Hispanic, Other] physician. This is my health, and I cannot afford to be politically correct.” As if unsubstantiated biases are merely politeness. Prejudice can be malicious hate or blindspot and implicit biases. In any form, a lack of JEDI weakens the health care delivery system causing pain and suffering for the community. Effective innovative leaders replace, “Not me, not us” with, “It could be me; it might be us” to ensure health care teams, organizations, and communities are just, equitable, diverse, and inclusive.
About the Author
Maureen Metcalf, Founder, CEO, and Board Chair of the Innovative Leadership Institute is a highly sought-after expert in anticipating and leveraging future business trends to transform organizations. She has captured her thirty years of experience and success in an award-winning series of books that are used by public, private, and academic organizations to align company-wide strategy, systems, and culture with innovative leadership techniques. As a preeminent change agent, Ms. Metcalf has set strategic direction and then transformed her client organizations to deliver significant business results such as increased profitability, cycle time reduction, improved quality, and increased employee effectiveness. She and the Innovative Leadership Institute have developed and certified hundreds of leaders who amplify their organizations’ impact across the world.
https://www.innovativeleadershipinstitute.com/wp-content/uploads/2021/05/Unsplash-Health-Care-DEI-by-Metcalf.jpg12801920Maureen Metcalfhttps://www.innovativeleadershipinstitute.com/wp-content/uploads/2022/03/ILI-Anniversary-Logo.pngMaureen Metcalf2021-06-07 11:31:082024-11-27 17:26:45Justice, Equity, Diversity, and Inclusion (JEDI) Innovative Health Care Leadership
This article is from the new book Innovative Leadership for Health Care. The book was written by Maureen Metcalf of Innovative Leadership Institute and several other co-authors, to provide healthcare workers with frameworks and tools based on the most current research in leadership, psychology, neuroscience, and physiology to help them update or innovate how they lead and build the practices necessary to continue to update their leadership skills. It is a companion to the podcast between Dr. Neil Grunberg, one of the co-authors, and Maureen titled Innovative Leadership for the Health Care Industry.
The Robert Wood Johnson Foundation’s Urban Institute reports that on an average night in the United States, around 465,000 people will go to sleep in our hospital beds. They will wear our gowns, eat food prepared in our kitchens, have their faces washed with water from our sinks. Some will undergo lifesaving procedures; some will undergo preventative observation, all will be in a state of vulnerability, unlike almost any other experience. Many will receive the care they would term as “miraculous.” Whether it is inside one of our 6,100 hospitals or in a rural office 100 miles from the nearest metro emergency room, health care is a big responsibility. It is always intimate. It is always humbling. It is often urgent.
Advances in training, education, information, public policy, and technology account for many of these daily miracles. We assert these miracles are also the result of extraordinary leadership. Leadership leveraging the strength of the team to go beyond the limitations of the individual. Leadership creating resources when and where they are needed. Leadership reaching beyond what can be touched and extending to the health care delivery system.
Just as receiving health care is intimate, humbling, and often urgent, so is leadership development. This book provides the education and tools to help you grow personally and increase your knowledge and skills. If you are not touched as well as challenged, lost as well as enlightened, and reflective as well as affirmed, then we have failed you. Leadership growth is a contact sport. Changing who you are is the real leadership growth that you seek. Creating miracles for your patients, staff, and community is your reward for risking this personal leadership journey.
Health care professionals are highly respected and valued in society. They have essential, existential roles as healers of the sick and injured and promoters of physical and mental health. Effective health care professionals apply their knowledge and skills appropriately and ethically. They respect colleagues, patients, patients’ significant others, and the limits of their knowledge and skills. They are leaders in that they are aspirational and inspirational. They influence these stakeholders and the organization’s cultures and systems in which they have a formal leadership role. They lead themselves, their people, their teams, and their organizations.
Becoming a better health care leader and optimizing innovation hinge on your ability to authentically examine your inner makeup and diligently address some challenging limitations. Leadership innovation or elevating your leadership quality can be accelerated by a structured process involving self-exploration, allowing you to enhance your leadership beyond tactical execution. While we provide a process, we want to be clear that readers should use this process to be effective for them. We each face different challenges and relate to leadership development in different ways. Each of us will use this book slightly differently. With that in mind, we tried to create a framework that is actionable and easy to follow. The process of leadership growth can be challenging, especially when it requires exploration of implicit beliefs and assumptions and potential changes to your overall worldview. Combining health care leadership with innovation requires you to transform the way you perceive yourself, others, and your role as a health care leader.
Wiley W. Souba noted, “Unless one knows how to lead one’s self, it would be presumptuous for anyone to be able to lead others effectively… Leading one’s self implies cultivating the skills and processes to experience a higher level of self-identity beyond one’s ordinary, reactive ego level… To get beyond their ‘ordinary, reactive ego,’ effective leaders relentlessly work on ‘unconcealing‘ the prevailing mental maps that they carry around in their heads. This unveiling is critical because leaders are more effective when they are not limited by their hidden frames of reference and taken-for-granted worldviews. This new way of understanding leadership requires that leaders spend more time learning about and leading themselves.”
By earnestly looking at your own experience—including motivations, inclinations, interpersonal skills, proficiencies, and worldview, and aligning them with the context in which you operate—you can optimize your effectiveness in the current dynamic environment. Through reflection, you learn to balance the hard skills you have acquired through experience with the introspection attained through in-depth examination—all the while setting the stage for further growth. In essence, you discover how to strategically and tactically innovate and elevate leadership the same way you innovate in other aspects of your profession.
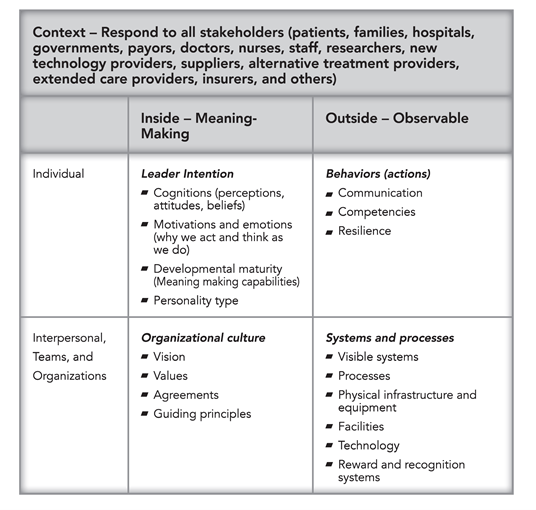
We define leadership using the following chart. Leaders must attend to and align all elements of the overall system continually to respond to changes within the system and external factors within your context, such as insurers and government regulations.
This table is foundational to depict how we talk about the facets of the leader’s self and organization. When one facet changes, the leader must realign other aspects to ensure efficient and effective operation. Many leadership programs focus on leadership behaviors; this book is different in that it addresses where the leader fits within the overall system and how they are responsible for leading.
The upper left quadrant reflects the inner meaning-making of each leader (the personal). It contains both innate and developed capacities. This quadrant provides the foundation of self-awareness and individual development. It serves as the basis for behavior, competence, and resilience. Leaders must be aware of their inner landscape to be truly effective.
The upper right quadrant reflects observable behaviors, actions, competencies, and communication. This quadrant is what we see in leaders. Leadership training often focuses on checklists of behaviors because they are easier to assess and discuss. This book is different; it suggests actions, but it is not prescriptive. We acknowledge that behaviors tie to your meaning-making, culture, systems, and processes.
The lower left quadrant is inside the groups (interpersonal/dyads, teams, and organizations). It includes the vision, values, agreements, guiding principles, and other factors that create health care cultures.
The lower right quadrant reflects the visible systems, processes, physical infrastructure and equipment, facilities, technology, and reward and recognition systems
Part of what is innovative about this approach is that it requires leaders to focus on all four areas concurrently. When one area changes, others are impacted. When leaders’ beliefs change, their behaviors often change. Behavior changes impact culture and systems. The same is true when the organization changes, such as shelter in place during a pandemic. Health care leaders need to change their behaviors and face new challenges, such as telemedicine’s increasing use. One essential leadership skill is to quickly realign across all four quadrants in response to changes in any single quadrant.
Innovative health care leaders influence by equally engaging their personal intention and action with the organization’s culture and systems to move the health care organization forward to improve the lives of the people it serves. These leaders also take into consideration the rightful interests of the organizational members. Depending on the role of leaders and sphere of influence, they impact individuals, teams, and the entire organization. Health care professionals who are innovative leaders adapt and develop themselves and their organizations to optimize effectiveness with changing environments or contexts (psychological, social, physical). This book guides health care professionals in becoming Innovative Health Care Leaders.
To find out more about this new book, Innovative Leadership for Health Care, click here. To find out how to implement this innovative book into your health system, contact Innovative Leadership Institute here
About the Authors
Maureen Metcalf, M.B.A., founder and CEO of the Innovative Leadership Institute, is a highly sought-after expert in anticipating and leveraging future business trends.
Erin S. Barry, M.S. is a Research Assistant Professor in the Department of Military and Emergency Medicine at the Uniformed Services University.
Dukagjin M. Blajak M.D., Ph. D. is an Associate Professor and H&N Division Director in the Radiation Oncology department at The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute.
Suzanna Fitzpatrick, D.N.P., ACNP-BC, FNP-BC, is a senior nurse practitioner at the University of Maryland Medical Center in Baltimore, Maryland.
Michael Morrow-Fox, M.B.A., ED.S., is a consultant with the Innovative Leadership Institute experienced in health care, education, banking, government, and non-profit management.
Neil Grunberg, Ph.D., is Professor of Military & Emergency Medicine, Medical & Clinical Psychology, and Neuroscience in the Uniformed Services University (USU) of the Health Sciences School of Medicine; Professor in the USU Graduate School of Nursing; and Director of Research and Development in the USU Leader and Leadership Education and Development (LEAD) program, Bethesda, Maryland.
https://www.innovativeleadershipinstitute.com/wp-content/uploads/2021/03/Innovative-Leadership-for-Health-Care-scaled.jpg17072560Maureen Metcalfhttps://www.innovativeleadershipinstitute.com/wp-content/uploads/2022/03/ILI-Anniversary-Logo.pngMaureen Metcalf2021-03-24 11:45:112024-12-02 13:00:00Innovative Leadership for the Health Care Industry